The scientists believe that switching to bivalirudin could save hundreds of thousands of lives each year.
Bivalirudin was discovered to be both safer and more effective than heparin in the treatment of heart attack patients undergoing percutaneous coronary intervention.
Recent research indicates that bivalirudin is a safer and more effective anticoagulant than heparin for treating patients with the most severe kind of heart attack who undergo urgent percutaneous coronary intervention (PCI), with a 31% reduction in the risk of mortality or major bleeding.


These are the results of a new study led by Mount Sinai’s Icahn School of Medicine researchers. This is the first large-scale clinical trial to examine the two anticoagulants most often used after PCI, and it demonstrates that bivalirudin given with a two- to four-hour high-dose infusion dramatically reduces thrombosis, major bleeding, and death when compared to heparin.


The results were recently announced in a Late Breaking Clinical Trial presentation at the American Heart Association’s Scientific Sessions (AHA 22) in Chicago and were published in The Lancet. This research might have far-reaching implications, altering the treatment of hundreds of thousands of patients worldwide who suffer a major blockage in a heart artery, a condition known as ST-segment elevation myocardial infarction, or STEMI. It is the most severe kind of heart attack.

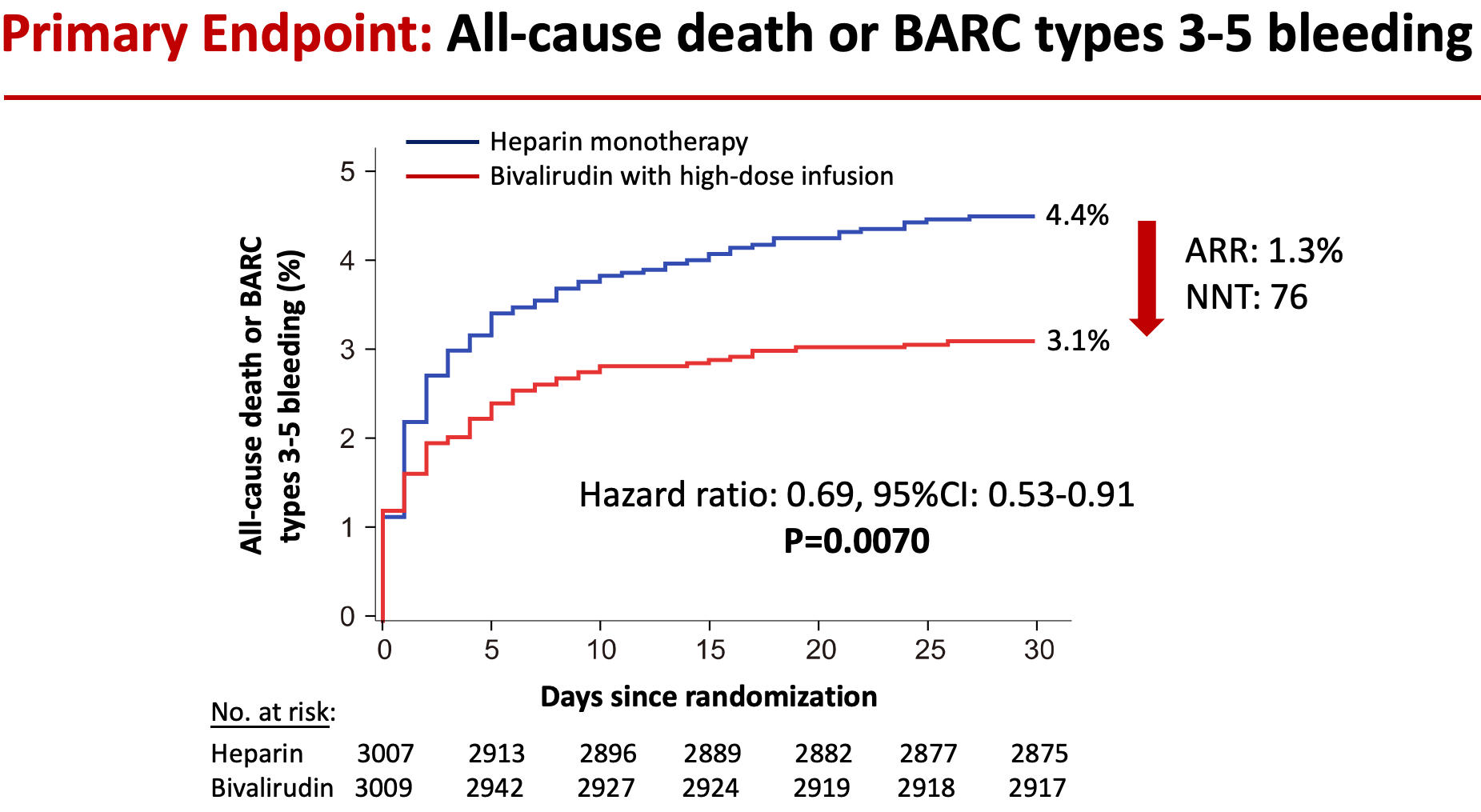
Reduction in the risk of death or major bleeding after primary PCI in patients with STEMI treated with heparin monotherapy (blue curve) or bivalirudin with a post-procedure infusion (red curve). The hazard ratio of 0.69 signifies a 31% reduction in risk. The ARR (absolute risk reduction) was 1.3%. The NNT (number of patients needed to treat to prevent one death or large bleed) was 76. Credit: Mount Sinai Health System
“For the first time, this study identifies the best and safest treatment course for patients undergoing stenting to treat a STEMI heart attack,” says co-Principal Investigator Gregg W. Stone, MD, Director of Academic Affairs for the Mount Sinai Health System and Professor of Medicine (Cardiology), and Population Health Science and Policy, at Icahn Mount Sinai. “Compared with heparin, bivalirudin plus a short infusion substantially improved the likelihood of surviving a STEMI and reduced the two most feared complications—major bleeding and stent thrombosis.”
Patients suffering STEMI heart attacks were included in the “BRIGHT-4” trial and received “primary PCI”—an emergency stenting procedure to maintain heart muscle function. During this minimally invasive operation, patients will need anticoagulant therapy to successfully open the blocked heart artery and prevent future blood clots from developing and triggering another heart attack.
The most common anticoagulant used during primary PCI is heparin. However, its effects can be somewhat unpredictable, leading to higher-than-desirable rates of bleeding and blood clots. Bivalirudin is a newer anticoagulant that has more predictable “blood thinning” effects. Heparin and bivalirudin have been compared in six prior large randomized trials in patients with STEMI, but in those studies, they were administered with varying regimens and background therapies. This new research evaluates the two most widely used regimens of heparin and bivalirudin, which have never been directly compared with each other in an adequately sized trial.
Dr. Stone along with Yaling Han, MD, Ph.D., of Shenyang Northern Hospital in Shenyang, China led a team of researchers to analyze 6,106 patients enrolled in the study across 87 sites in China between February 2019 and April 2022. All underwent primary PCI for STEMI treatment, nearly all with a procedure that used the radial artery in the wrist to target the blocked heart artery. Patients were randomized to receive the two most widely used regimens of heparin and bivalirudin, which prior studies have shown to be the safest and most effective. One group received heparin alone, administered through an IV. The other group received bivalirudin through an IV, followed by a high-dose IV infusion for two to four hours after the procedure.
Investigators followed patients for 30 days following the procedure, the timeframe in which STEMI patients are at the highest risk for adverse events. The primary goal of the study was to compare the occurrence of all-cause mortality or major bleeding. Researchers found that 4.4 percent of patients treated with heparin died or had a major bleed within 30 days, compared to 3.1 percent of patients treated with bivalirudin. Overall, the bivalirudin group had a 31 percent reduction in the rate of death or major bleeding compared with patients in the heparin group—a highly statistically significant reduction.
The researchers then looked at the specific incidence of death alone and major bleeding alone between the groups. They found that deaths were reduced from 3.9 percent in heparin-treated patients to 3.0 percent in bivalirudin-treated patients. Severe bleeding also was reduced from 0.8 percent in the heparin group to 0.2 percent in the bivalirudin group. Both of these differences were statistically significant.
They also analyzed the rate of stent thrombosis—a complication that happens when the vessel abruptly closes as the result of a blood clot that typically leads to a second heart attack or death. This was also lower in the bivalirudin group at 0.4 percent compared with 1.1 in the heparin group, again a statistically significant reduction.
“These results are dramatic,” Dr. Stone said. “The simple decision to use bivalirudin during primary PCI in patients with heart attacks, which is now generic and thus inexpensive, can save hundreds of thousands of lives per year and prevent major bleeding and stent thrombosis compared with heparin.”
Reference: “Bivalirudin plus a high-dose infusion versus heparin monotherapy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: a randomised trial” by Yi Li, MD, Zhenyang Liang, MD, Lei Qin, MD, Professor Mian Wang, MD, Xianzhao Wang, MD, Huanyi Zhang, MD, Yin Liu, MD, Professor Yan Li, MD, Zhisheng Jia, MD, Professor Limin Liu, MD, Professor Hongyan Zhang, MD, Jun Luo, MD, Songwu Dong, MD, Professor Jincheng Guo, MD, Hengqing Zhu, MD, Shengli Li, MD, Haijun Zheng, MD, Professor Lijun Liu, MD, Professor Yanqing Wu, MD, Professor Yiming Zhong, MD, Miaohan Qiu, MD, Professor Yaling Han, MD and Professor Gregg W Stone, MD, 6 November 2022, The Lancet.
DOI: 10.1016/S0140-6736(22)01999-7
The BRIGHT-4 trial was an investigator-sponsored and organized trial. The trial was funded by the Chinese Society of Cardiology Foundation with a research grant from Jiangsu Hengrui Pharmaceuticals Co., Ltd.